30 May 2026
8min read
Contents

ED isn't only a condition of older men. The causes, and what 'normal' actually looks like, change significantly with age. A 30-year-old struggling occasionally has a different conversation to a 70-year-old. This guide is the LYV Clinical Team's age-by-age summary of what to expect, what's common, and when to seek help.
Erectile dysfunction at different ages is one of the most searched topics for men looking for discreet online ED treatment in the UK. Some men want to know whether occasional erectile difficulty in their 30s is normal. Others want to understand why erections change in their 40s, 50s, 60s or 70s. The answer is not the same for everyone, because erectile function is affected by age, stress, blood flow, hormones, medication, lifestyle, and overall health.
The most important point is that ED can happen at any age, but persistent erectile dysfunction should not be ignored. In younger men it is often linked with stress, anxiety, alcohol, sleep and relationship factors. In older men it is more commonly linked with vascular health, diabetes, blood pressure, cholesterol, prostate symptoms and medication use. Understanding the pattern helps a prescriber recommend the safest and most suitable treatment.
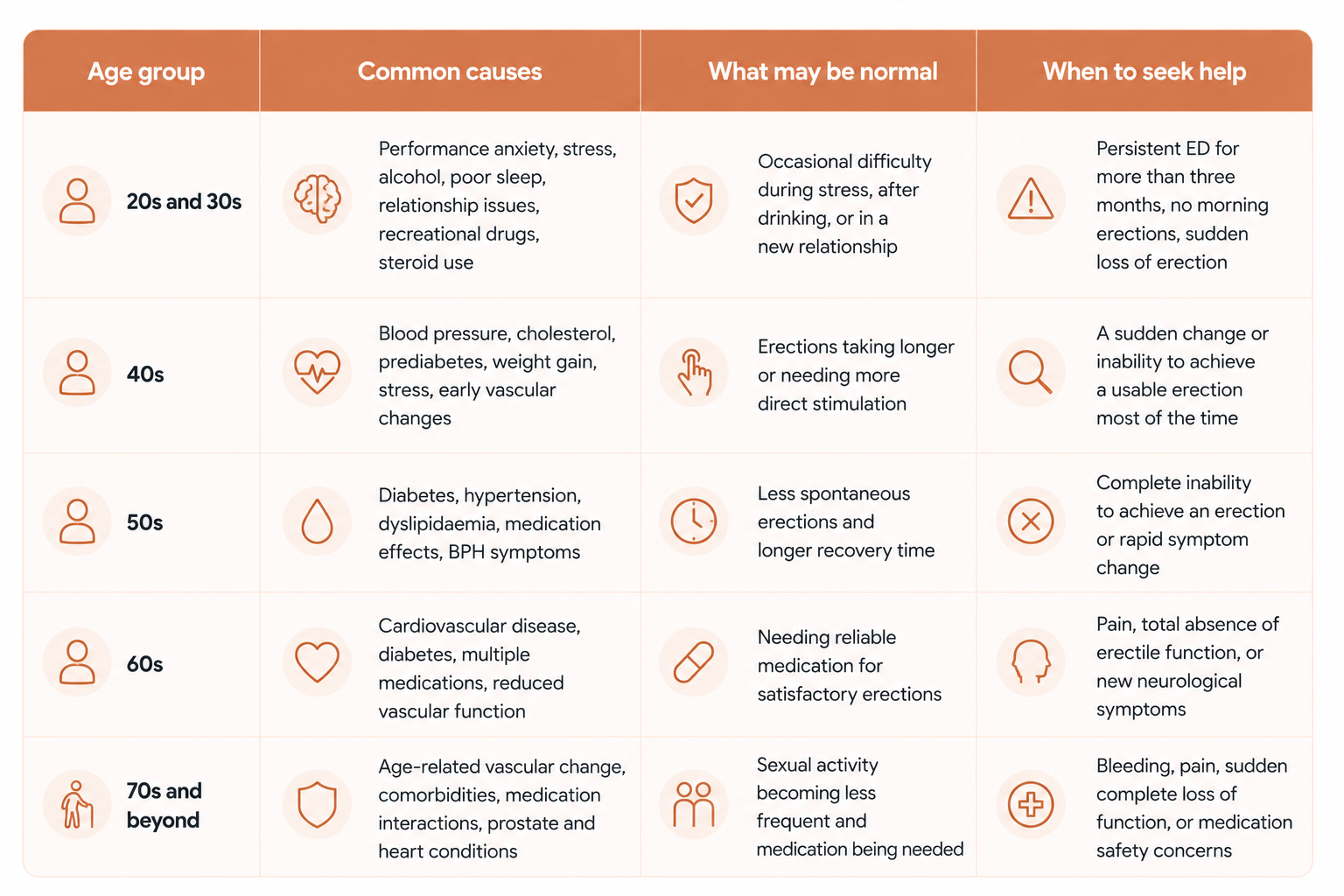
Erectile dysfunction in younger men is more common than the cultural narrative suggests — UK data shows that around 1 in 4 men under 40 have experienced ED at some point. The causes at this age tend to be different from older men. Psychological factors are dominant: performance anxiety, stress, depression, relationship issues, the after-effects of an embarrassing first episode. Lifestyle factors come next — recreational drug use, alcohol, sleep deprivation, very high pornography consumption, and steroid use. Vascular causes are rare but worth screening for in any man under 40 with persistent ED, particularly with a family history of early heart disease.
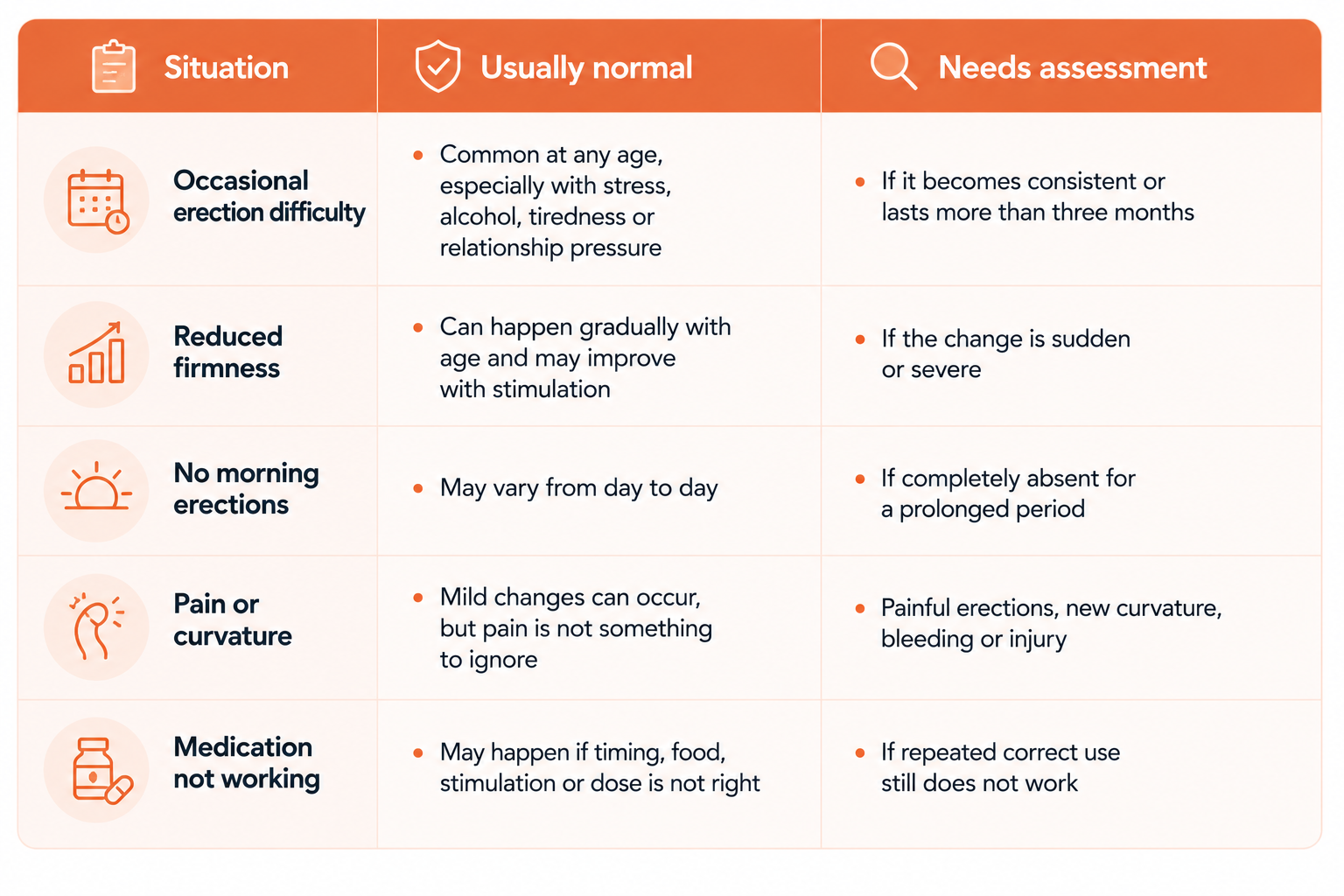
What's 'normal' at this age: occasional difficulty after a long night, when stressed, or in a new relationship. What's not normal: persistent difficulty over more than three months, total absence of morning erections, or rapid loss of erection mid-encounter. If those apply, it's worth getting it looked at properly rather than waiting for it to resolve on its own.
For men in their 20s and 30s, ED can feel especially worrying because it may seem unexpected. However, temporary erection problems are very common when stress, anxiety, alcohol, poor sleep or pressure around sexual performance are involved. The pattern matters. A one-off episode is very different from a repeated issue that affects confidence, relationships or quality of life.

The 40s is the decade where vascular and metabolic causes start to take over from psychological ones. Hypertension, prediabetes, rising cholesterol, and weight gain begin to affect the small blood vessels of the penis years before they affect the larger ones in the heart. ED in your 40s should always trigger a cardiovascular risk assessment — blood pressure, cholesterol, fasting glucose, BMI. The treatment is usually a combination of lifestyle change and PDE5 inhibitors, with the lifestyle side doing most of the long-term work.
What's 'normal' at this age: erections may take longer to develop, be slightly less rigid, and require more direct stimulation. What's not normal: inability to achieve a usable erection most of the time, or a sudden change without obvious cause.
For UK men searching for erectile dysfunction in your 40s, the key message is that ED can sometimes be an early warning sign of wider health changes. Because the blood vessels in the penis are small, erection changes can appear before symptoms elsewhere. This does not mean every case is serious, but it does mean persistent ED is worth reviewing properly.

By the 50s, around half of UK men report some degree of ED. Vascular causes dominate, and metabolic comorbidity (diabetes, hypertension, dyslipidaemia) is common. Many men in this decade are on at least one medication that can contribute (beta-blockers, statins, SSRIs, prostate medications). Treatment is usually straightforward: address modifiable risk factors, switch any contributing medications where possible, and use PDE5 inhibitors as needed. The 50s is also when daily-dose tadalafil starts to become a more popular option because of its dual benefit on BPH symptoms in men starting to develop urinary frequency.
What's 'normal' at this age: less spontaneous, somewhat firmer with direct stimulation, recovery time between erections is longer. What's not normal: complete inability to achieve an erection, or symptoms changing rapidly without an obvious trigger.
Men in their 50s often compare sildenafil and tadalafil because both are commonly prescribed for ED treatment in the UK. Sildenafil may suit men who prefer planned intimacy, while tadalafil may suit men who want a longer treatment window or who also experience mild urinary symptoms. A prescriber can help decide which option fits best with current health, existing medication and lifestyle.
By 60, around two-thirds of UK men report some degree of ED. The picture becomes more complex because comorbidity is the rule rather than the exception, and the contributing medications add up. Diabetes and cardiovascular disease are now common. The treatment principles are the same — address risk factors, review medications, use PDE5 inhibitors — but the medication choice may need more careful consideration of interactions and dose.
What's 'normal' at this age: needing reliable medication for satisfactory erections; longer recovery between sexual encounters; sometimes a longer time to climax. What's not normal: total absence of any erectile function with stimulation, or significant pain with erections (which can suggest Peyronie's disease and warrants specialist review).
ED in your 60s should be approached with both confidence and caution. Many men respond well to oral ED medication, but the prescriber needs to consider blood pressure, heart disease, diabetes, prostate medication and any nitrate use. This is why a proper clinical assessment is important before starting or changing treatment.

ED is the rule rather than the exception over 70 — somewhere around 70–80% of UK men in this age bracket have meaningful ED. This does not mean a satisfying sexual life is over. PDE5 inhibitors remain effective and are widely prescribed in this age group, with attention to interactions, particularly nitrates. Many men in their 70s and 80s are using these medications happily for years. Frank conversation with a prescriber matters more than ever — about what you want from treatment and what fits your overall health picture.
What's 'normal' at this age: needing medication for satisfactory function; sexual activity less frequent; orgasm intensity may be lower. What's not normal: bleeding, pain, sudden complete loss of function, or any change associated with new neurological symptoms.
For men over 70, the goal of ED treatment is not only erection quality. It is also comfort, safety, confidence and quality of life. Treatment may still be appropriate, but it should be matched carefully with overall health and existing medications.
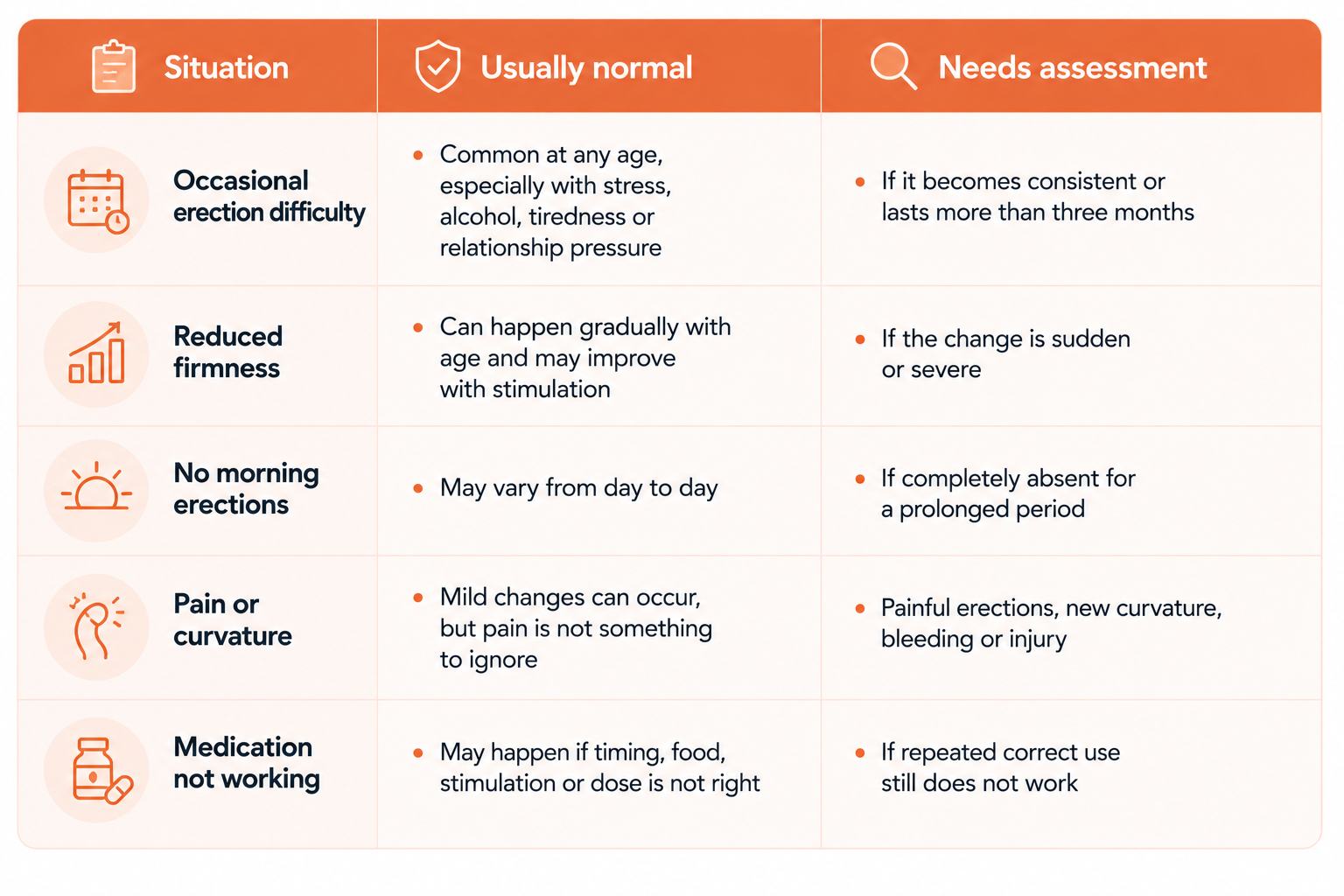
If PDE5 inhibitors don't work despite a properly trialled dose, or if the response has faded over time despite no other obvious change, second-line options exist — alprostadil (intracavernosal or urethral), vacuum erection devices, and in some cases penile implants. These are specialist routes, usually accessed via GP referral to urology. They are genuinely effective for men who don't respond to oral medications, and the conversation is worth having rather than assuming nothing further can be done.
Medication can help many men, but ED treatment works best when it is part of a broader health review. Blood pressure, diabetes risk, cholesterol, weight, smoking, alcohol intake, sleep and mental health can all affect erectile function. Improving these factors may also improve long-term sexual health and general wellbeing.

LYV's online ED consultation is reviewed by a UK GPhC-registered prescriber. We'll recommend the right treatment for your age, health and lifestyle — or recommend a GP visit if that's the right next step.
Whether you are experiencing ED in your 30s, noticing changes in your 40s or 50s, or looking for safe erectile dysfunction treatment later in life, a confidential clinical review can help identify the most suitable option.
This article is general information for UK adults and is not a substitute for personalised medical advice. Prescription-only medicines mentioned are dispensed only after a clinician-led online consultation through LYV Pharmacy (GPhC registration 9012803). If you have concerns about your symptoms or any medication you are taking, speak to your GP or call NHS 111.
Author
